Tulsa City Council Urban and Economic Development Committee Meeting - April 22, 2026
STREAMING COPY IN PREPARATION — RECORDING AVAILABLE FROM THE ORIGINAL SOURCE
How quiet everybody is.
We're live.
All right, good morning, everybody.
It's 10 30 in the morning, April 22nd, and this is the Tulsa City Council Urban and Economic Development Committee meeting.
My name's Anthony Archie from Council District number two.
First item of business is to call this meeting to order.
Second order of business.
The ordinance naming increment district E of the amended and restated Tulsa International Airport Economic Uh Development Plan as Incentive District Number 26.
City of Tulsa and establishing the date for the creation thereof, ratifying and confirming the actions recommendations and findings of review committee and the Tulsa Metropolitan Area Planning Commission with regard to increment district E ratifying and confirming the action of the City of Tulsa in enacting ordinance number 23475.
I need to continue on, probably.
Sarah's not here.
I'll keep on reading.
No, it's fine.
Okay.
No, yes.
You stop wherever you have to do that.
Okay, you just have to summarize what's there.
Great.
You don't even have to read it.
We're adding to the um to the plan.
Okay, so Alex and Jeff are here with us.
Thank you for being here.
Good morning.
Thank you for having us.
So we are officially requesting permission to trigger our fifth and final TIFF district, which is within our project plan.
Um it's exciting to be able to trigger it because we already have a company that is starting to develop the Agile Space Industries group groundbreaking that we had earlier this year is within this district.
And so this is a combined property tax and sales tax generation district.
So as they start construction on that, any um taxes they paid, we can partner with the state in order to receive some of those funds back and use those funds for future airport development.
But it's about 1500 acres, right, Jeff?
Yep.
Um of our about 4900 acres that we have at Tulsa International.
Well any questions.
How many acres?
1500.
Yeah.
49.
Great.
Well, thank you for the work that you're all doing.
Let's expand the tip.
Okay.
I have something real quick.
Oh, please.
Thank you for all your hard work out there at the airport.
Really do appreciate it, but thank you for bringing Alaska Air.
You're doing really well.
So fine.
Yeah.
Sure.
Jeff, did you want to say anything?
No, I just the statutory deadline for activating this TIFF is June 16th.
So definitely will act on it before then.
All right, thank you all so much.
All right, item number three.
Let's talk about Kendall Whittier.
Resolution directing the filing of the annual assessment role for the Kendall Whittier.
Improvement district number one assessment role with the Tulsa City Clerk.
Setting June 10th, 2026 as the date of public hearing on the notice of the role and directing this resolution and notice of public hearing to be published two times.
All right, Samantha's with us.
Yeah, hi Sam.
I stands with the planning office.
Um so this is a renewal of the bid.
It is in its sunset year, so it's last year.
Um it will end in assessments will end in June of 2027.
Um changes from the role from last year to this year.
One property's physical address changed, so that doesn't really change much.
And then three property zoning changed from commercial to residential, um, and thereby we're exempted from assessment.
So that reduces the annual budget of the assessments by uh 1,030 and 11 cents.
So the total now that the um annual assessment um generates is 47,604.31 cents.
That's a flat rate for um businesses.
So what they paid last year, they're paying this year.
And just as a reminder, the improvements that that funds is landscaping and trash removal, security services, beautification, lighting, parking lot repairs, and then administration.
All right.
Any questions or concerns?
All right.
Thank you, Sam, for being here.
Okay, um, there is some amended language on item number four.
So I'm gonna read the amended language.
Um resolution approving the allocation of affordable housing trust funds in the amount not to exceed 269,408 to assist in construction rehabilitation and improvements, including 147 affordable housing units pursuant to the agreement to provide development assistance for affordable housing trust funds between the city of Tulsa and Tayo in accordance with the economic development policies of the city of Tulsa Oklahoma.
Aaron is with us.
I am with you.
I'm gonna lean on Councillor Gilbert's third district for the Oyo Hotel, which takes the hotel and puts the former housing into that.
Well, I had I had no idea.
You had no idea.
I had no idea.
Oh wow, okay.
So you're kidding.
No.
Who's working on those?
This was this came through our former housing trust funds for TO.
This is the one off of I 44.
Yes, that's the umbody nobody's told me anything about this.
You should have been on it, please.
Um I apologize.
What I would like to do if you don't mind is table this item to make sure that we have the counselor fully uh aware of what is going on.
I apologize that you were not involved on this project.
So Sarah will just put it on for just put it on for committee news.
It can always be pulled off the five o'clock.
Okay, okay.
Is it through economic development?
Sorry.
Please go ahead.
So through economic development or housing.
A former housing trust went through too.
Is that Vicky Jordan?
That's Vicky Jordan, yes.
Okay.
So it would have gone through the review committee, which I'm surprised if you want to.
Are you sure it's in district five?
Yeah, it's um I 40.
We have that too, right?
On borders.
But does anybody know about it?
No, I didn't know I just wasn't share it.
We share yale.
Yeah.
Oh, so probably both should.
This is just an update.
Yeah.
I mean, my full apologies for that.
Oh, you don't want to find that situation, and we will get back to you on that.
So these are governed by an economic incentive policy that requires a re-drow technical committee and then full review committee.
Okay.
And so, and then it comes.
And then it comes to the council.
So the district counselors and the full review committee.
That's why I'm surprised that you didn't know because you're supposed to be in the preview committee.
All right.
Thank you, Aaron, and I don't work for the apologies.
I know.
Oh, that's all right.
Thank you, sir.
Well, thank you, we appreciate you.
Okay, well then we will uh kick this uh to next week.
Let's go to item number five.
Let's talk about IMSA.
Discussion with representatives from IMSA, emergency medical services authority regarding IMSA's transport, rate alignment, and treatment in place proposals.
All right, MSA's here.
Good morning, Council.
Uh Johnny Easy with EMSA.
Thank you so much for having us this morning.
I do believe that you provided all the backup documents prior to this meeting.
We also have them for you if you'd like them.
Uh just to take one and pass around so we can make notes.
Um I'll start off with uh why we're here.
First and foremost, I first and foremost, um, I'm bringing to council really two things today.
Um we are asking council in May uh on council agenda to approve a rate alignment whereby MC update our current transport rates and bifurcate our rates out in a structure that reflects level of care provided, and then the second resolution would be to implement a treatment in place uh fee.
Um I do want to be really clear.
Um, this is not a request, nor in any way uh are we asking council to even consider an increase in EMSA care rates.
In fact, this would do exactly opposite of that.
Our goal uh is to preserve uh fund 121 to ensure your EMS system has long-term sustainability.
So the way that we do that is to maximize third party revenue, so getting insurance providers to pay um what uh what is owed on behalf of the patient.
Um that means that the patient is paying as little out of pocket as possible, and that we're able to cover operational costs without seeking uh fund distribution from the EMSIC care subscription fund.
So I I just wanted to set the stage for that really clearly.
Um also um this we've been working on this proposal for a couple of years.
So yeah, I'm gonna turn this slide over to you so that you can talk just a little bit.
Again, we'll go into the rate alignment proposal, so that's our base rates and our bifurcation, and then we'll switch over into the transport.
I'm sorry, the treatment and place fee.
All right.
So as Jenna outlined, this is our proposal in a nutshell.
We're going to update our base rates to reflect the level of service, which could potentially bring in 1.9 million dollars in additional revenue reimbursement just from the rate alignment alone.
The uh treatment in place rate of 500.
We estimate that that will bring in an additional 1.6 million dollars for that service if we start to charge for it.
And then the third part of our proposal is to implement a 40% uninsured discount to help defray any impact of rate alignment to our uninsured patients.
And then the table shows you the charges, EMSA's current rates and what we are proposing.
The two highlighted items are our highly utilized services.
The last item there, the specialty care transports, that is less than one percent of our services.
We know that that seems like a significant increase from $1,300 to 2800.
However, those are higher level of services, and so we believe that adjusting our rates to reflect the level of services that we provide is appropriate, and those are typically reimbursed by facilities, hospitals because those are interfacility transports.
Well, well, I can wait till you guys are done, and I'm just getting in the queue.
Okay, so he's chairing the meeting, so we'll put our fingers up so he can do it.
Okay, we don't have just ignore it.
Yeah, we'll do all of it.
And that's a little disruptive.
Welcome.
So we just want to outline what changes and what space is saying.
What's going to change is that EMSA is going to update our emergency transport rates for the first time since 2012, as well as implement the 40% uninsured discount, which will be happening for the first time.
We're going to expand our charge master to appropriately bill for the care that we provide.
Um and recovered costs that are currently reimbursed by private insurers and Medicaid.
Our state Medicaid has provided payment and reimbursement for treatment in place since 2011.
EMSA has not been able to recover those costs because we did not charge for it.
We did not have a charge in place for it.
What's going to stay the same are MSI care members will continue to pay zero out-of-pocket costs, and this will not affect them because any out of pocket is covered by the EMSA care benefits.
This will not change our mission, our operational structure, or the way we dispatch and respond.
Treatment in place will also be covered by EMSACare benefits, and we are proposing not to charge uninsured patients for treatment in place for the first two-year period so we can gather utilization data.
And EMSA continues to remain the lowest, the lowest cost EMS provider in the state of Oklahoma year over year.
So the goal of the two-year moratorium for uninsured is to really understand.
We've been studying the data of our patient population for a really long time.
But we want to make sure, you know, when you make any change, we want to make sure that there's not a higher utilization than expected, or that we don't see a decrease in 911 utilization.
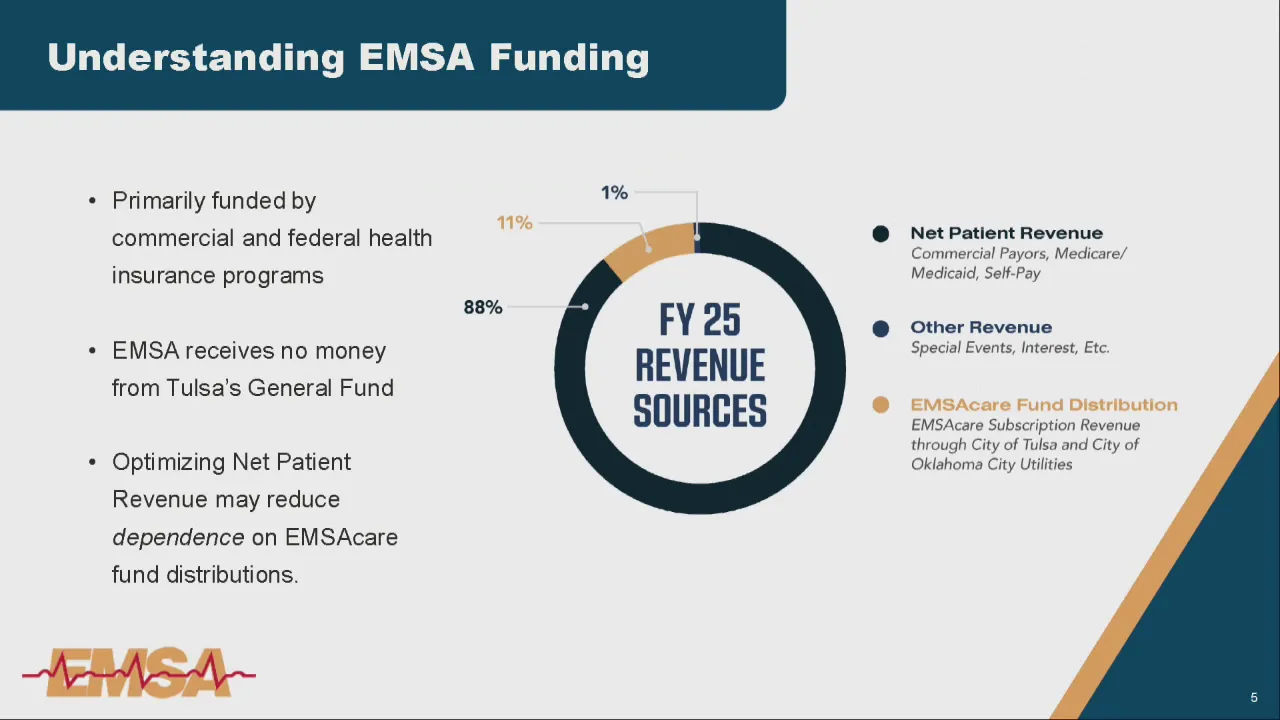
So the next two slides are really just uh basic reminders for councils that the majority of our revenue does come from net patient revenue.
So that's revenue that that's reimbursement that we are seeking from commercial payers, Medicaid, and Medicare primarily.
Um, Medicaid and Medicare.
As you all know, um, that really depends on current administration and administration budget at the federal level.
And so we brace for impact for those every single year, as we are currently bracing for impact from proposed changes in Medicaid.
So our goal really is to look at this rate alignment proposal to ensure that we are now really and appropriately putting the value on the care provided, meaning that you know, back in the day, uh CMS had a few HICS-PIX codes or a few codes by which you charge for services.
Obviously, over the years that has expanded.
We have not expanded that.
So if it's an emergency ALS or BLS, we charge one rate no matter what intervention is provided.
And so if you know, if you require whole blood, right now we can charge at a higher rate for that.
Uh whole blood costs us about $500 per unit.
Um, where and it puts it in a higher level of care.
If you don't require an intervention like that, obviously the care uh is fee-based, so it's at a lower level.
So I just want to be really clear, we are not changing the way we provide care.
We're really just um bifurcating out our levels of care so that it reflects what's being provided on scene.
If you want to run to the next slide, so um, I just want to I don't we can go to the previous slide.
So one of as Jonah mentioned, we're really trying to maximize our reimbursement from the commercial payers.
Um, Oklahoma passed a balance billing law which tied reimbursement in either to the lesser of locally approved rates or 325% of Medicare.
Now, most insurance providers prefer the 325% of Medicare because that is typically lower than what providers uh approved rates are, except for EMSA.
Go to the next slide, please.
So EMSA, these are EMSA's current rates, and um the last column shows you the 325% of Medicare's rates, so that is a negative that we could make up if we adjust our rates as compared to what it currently is.
So basically, what we're saying in this slide is that uh insurance companies have actually adjusted their charge masters long before we adjusted ours, and um they're actually reimbursing at a higher rate than we're charging.
So they recognize uh the need um to increase a reimbursement, and um we're just a little behind the game.
So we're leaving this money on the table.
We are leaving this money on the table.
Yeah, that was in the world for question, counselor.
I just wanted everybody to know in other words.
Are you still the chair of the trust?
No.
Are you still on the trust?
Yes.
Okay.
The authority.
Okay.
Yeah.
Thank you.
So since again, we haven't updated our rates since 2012, and what we have seen across the health care industry is a 48% or 43%, I'm sorry, 43% inflation rate.
So since uh 2020, um, EMSA directly has seen a 55% increase in our costs to procure ambulances.
We've increased our wage and compensation to all frontline providers by approximately 32%.
Our capital equipment and supply costs have gone up 25 to 30 percent.
And so again, as counselor Lakin mentioned, um, you know, we we do have opportunity uh to recoup costs by third-party payers.
Um, as always, our goal is quality patient care.
Um, this again does not change our model.
Um, our goal will be to recoup as much as we can from insurance providers, whereby our patients will pay as little out of pocket as possible.
Right, so we um did a comparative analysis, we looked at cost of the same services.
We compared organizations across the country, and we also looked at organizations around us, so um our neighbors, and this is where EMSO's proposal lies compared to some of the other communities around us.
Okay, uh we have some pension perspectives here because we as one of EMSA's uh value is being a patient centered, and so we wanted to look through the eyes of the patient to see what this would look like for the patient.
So we have a patient example and we kind of outline what that would look like if the patient is an MSACAR member, if they're not an MSA care member, they're uninsured.
The bottom line is that if they are an MSA care member, they will see no changes with our rate alignment.
If they are insured but not an EMSA care member, then they will pay whatever their insurance determines their co-pay is, which typically is determined again by their insurance company and a contract, and then if they're uninsured, they will actually see a reduction compared to our current rates with the implementation of that 40% discount.
So just going over looking deeper into treatment in place, again, just reiterating what Jonna has said.
Treatment in place is not community paramedicine.
It's not a new line of service that MSA is proposing.
These are emergency requests for services that we already respond to, but the patients decide that they don't want to be transported, we just don't have a way to capture that specific reimbursement.
Typically occurs when patients call 911, we complete an assessment and we provide treatment.
So an intervention is necessary in order for this, and then patients can refuse to be transported to the hospital.
We estimate that for Tulsa, we spend about seven million dollars and only providing the treatment in place services, and we have the ability again to get reimbursed 1.6 million dollars.
This is just some data showing how we got to that number of the anticipated revenue compared to our annual responses.
Again, a patient uh perspective for treatment in place if they are an MC care member, and so care benefits recover any out-of-pocket they might have if they are insured and not an MC care member, then um if we have a contract with their insured, then they will prohibit us from waiving any out-of-pocket costs, and if they are uninsured, we are proposing waiving um all out-of-pocket costs for a two-year period.
So, just uh and to summarize everything we've talked about.
I think it's uh everyone has been listening to the news.
We hear a lot about Medicare and Medicaid reimbursement, um, and the the uh health care uh financial struggles that everyone is experiencing both hospitals and including EMS as well, because the reimbursement is always at risk, and they reimburse below the cost of providing the services.
We actually have already seen some impact in that where our uninsured population is increasing, um, and which will lead to uncompensated care.
So, again, our charges are lower, um, and because our base rates have not been changed since 2012, we are now basically under billing for our services, and um they reimbursement that we stand to get from that.
So, Jonathan.
Yeah, I think just to wrap it up, um, again, I want to want to be really clear.
Um, no change to EMSA care.
Um, our goal uh is to be um for long-term sustainability of your EMS system.
So you included fund 121.
Um, we have not um our draw on fund 121.
Uh my goal is to decrease it every year.
It has been flat for the past three years, um, even though operational costs have gone up.
This is just additional revenue uh that is available to us that would then require us to rely on the sources.
Happy to answer questions.
For sure, we have a little bit of a cue.
So saw Councillor Bellis's hand go up.
Counselor Gilbert, were you did you put your hand up over there?
I did not.
Okay, good.
Okay.
So after Bellis, we'll have debts and then counselor um Dr.
Wright.
Yeah, I um just had a few clarifying questions about um some of like the rates, which I totally makes sense to go, hey, we weren't able to capture this from our because we weren't billing for it.
Um, I was curious, do you all though?
And I'm so sorry if you said this and I missed it.
Do you all have a difference between what's billed to insurers versus out of pocket rates?
Like, for instance, when you're I wasn't sure if this because I know sometimes, like you know, in a hospital setting, right?
For example, they would be like, hey, this is what we would charge someone if they're paying like cash versus what would be billed to an insurer, so there's not a difference there.
No, um, and that is because our rates are approved by our board, but set by council.
So we um okay.
Is that something that's feasible though if it was approved?
I'm just this is just a curiosity because I know other medical settings that do that difference between hey, we could get this from insurers if we build up to this level, like that's what they're you know, like whatever whether it's Medicaid reimbursement or otherwise, versus hey, if someone had to pay out of pocket, this is the flat rate we charge them.
Yeah, so that's um what we're doing is what is typical in the health care industry of work in a healthcare organization, um hospital system before, and what they do, the patients don't see it, but it's exactly what we're doing where there's a set charge and then there's a discount that is applied after the fact, and they just calculate the discount to that becomes that kind of out of pocket rate.
I assume that's helpful.
That's what I was kind of curious if that was operating that way.
Okay, that's helpful.
Okay that's helpful and then for your calculations I like I appreciated also that kind of like that two-year moratorium which also kind of fits with some of the federal and state level Medicaid and stability is that part of your all's calculations budget wise where should we see more significant cuts to Medicaid and thereby a lot more uninsured folks within the region like does that 40% still math for like if you're doing that kind of discount rate and you have more people that are paying out of pocket does that still does that math still work for you all to yeah so there the answer is yes um and two reasons number one we wanted to make sure that um we are preserving the value of EMSA care excuse me and so our 40% um uh I'm sorry forty percent reduction uh is comparable to what we offer in current EMSA care we go into every year uh projecting what you know based on what we're hearing what the chatter is and what we're seeing uh across the industry um projecting a variety of cuts to our uh government payers so we look at that every year um I think we're very conservative in our budgeting practices for that reason um and our trustees um know that as we bring our budget forward um that there are our major payer right is the most volatile so we would be um irresponsible not to consider what that would do in an annual fiscal year yeah that makes sense um and then just as a uh last question related to the treatment and base concept I'm curious what the like delineation is there like one I'm curious about why it was zero before which I'm glad you guys are you know seeking to get that revenue but then two for just as an example I think there have been there's been a time where I called 911 because I saw someone who was unhoused outside and I couldn't tell if they were alive or not right CRT or whoever wasn't showing up I was a little reticent to disturb them if they were just asleep but I thought they might need medical care if they've been outside that long in the cold um and so EMSA shows up folks you know team hops out of the ambulance real quick checks the person wakes up and goes away and I can tell that probably happens a lot actually you know they were used to showing up and going oh actually this person's fine they just like needed to wake up and go inside somewhere worm probably is that like that's not really you but you did have to go out there so I just wasn't sure at what point it's we're rendering treatment sure like so it's not that no so uh treatment in place really is um has parameters established by CMS so treatment requires treatment so if we come out and we do an assessment on a patient and the patient says I'm good um then you know they sign a refusal just like they do now like if we provide intervention so um think about um you know maybe you are a diabetic or the patient is diabetic um we do Ivy intervention with dextrose and the patient says you know what I am a brittle diabetic my wife's in the other room I'm gonna I'm gonna eat and I'll check in with my primary care we now we leave uh after care instructions we encourage the patient to call 911 again should their condition worsen and we leave um in this case that patient because we did do intervention we provided medical care that we are not able to recover costs from so I hope that answered your first question did so it's just to clarify this you mentioned so you could do an assessment and that wouldn't be treatment which I get that that's different than treatment I just wasn't sure what at what point you had a trigger into being able to bill and reimburse versus okay so intervention is what we call it and so if we're doing intervention um if you know um rendering actual medical care um that's when we would trigger in the TIP um I think you asked another question no I think that actually covered I was just I was just making sure I understood at what point it would then be something you can bill for which you yeah because like for instance that is like or you know also just for the public office too so someone could show up and help like take someone's heart rate and do some basic checks and that's not correct okay but it's at the point that you're administering some type of care.
Yes okay and I actually think your question was why have we why is it going to be why was it zero yeah yeah so uh a couple of things treatment in place is you know in terms of health care billy um relatively new it's only been around in the EMS world for you know maybe 10 to 15 years um there are some insurance providers that um like state Medicaid that recognizes it is much cheaper for them to and more feasible for them to pay a treatment in place fee than for their um enrollee uh to go to the hospital and have emergency care or have an emergency bill so um it's relatively new in the EMS world number one number two um we simply haven't had a fee structure in place in in EMSA to be able to do it uh why have we not brought this before I my honest answer is number one I've only been the CEO for four and a half years so I can only tell you about the last four and a half years and our focus um was really making sure that we were doing everything we could from a reimbursement perspective a process of
So um it's relatively new in the EMS world, number one.
Number two, um, we simply haven't had a fee structure in place in in EMSA to be able to do it.
Uh why have we not brought this before?
I my honest answer is number one, I've only been the CEO for four and a half years, so I can only tell you about the last four and a half years.
And our focus um was really making sure that we were doing everything we could from a reimbursement perspective, a process improvement perspective to make sure that we had everything under control, and that we didn't leave that it wasn't anything on our side that we could do.
Um, and then we started to identify now here are the other ways and the other opportunities for us to seek revenue.
Actually, that's one last clarifying question from that.
Is that kind of so Adam Crassy?
Is there when you're administering treatment in place?
Is that kind of like a bundled fee for whatever happens there, or can you also then bill for what actually gets administered more specifically on top of that, or how does that so we only have one set rate so right now?
So if it's an A, so in our current fee, if it's um ALS emergency, it's $1,300.
We get we get reimbursed that if the patient gets transported, it doesn't matter, it doesn't matter what we do on scene.
Okay, and this would be the same.
Okay, thanks.
That's helpful.
So we don't we're not itemizing, so for every you know, for every uh blood pressure cuff for every needle for every thing, uh it's not idle.
Okay, thanks so much.
Yes, all right, counselor Dutton and Counselor Wright.
So I'm looking at the percentage of coverage by Medicare, Medicaid Medicare, Advantage, Medicaid and Manage Medicaid, and that's a total of like 71% from the graph here.
And there are multiple bills at the Capitol right now that are looking to cut funding for citizens and leaving the uh Medicare and Medicaid into the hands of legislators in Oklahoma City.
And so I was looking at the number of uninsured in Tulsa, and it looks like we have 27.4% uninsured, 29.4% uninsured population that is dependent on the Medicare and Medicaid, possibly, and then 28.3% Hispanic population.
So that's those are kind of high percents.
What's going to happen after the two-year term of uh treatment in place pilot that's going to be implemented?
So the goal for the two-year moratorium is really for us to ensure you know, when you make a change in fee structure or you make a change in in operations, um, there needs to be a window of opportunity to make sure you don't have any unintended unintended consequences, right?
So again, we have years and years of patient population and um dispatch transport data.
What we're wanting to make sure is that um by implementation of a fee that we're not seeing either an underutilization in that particular dispatch code or in that that particular patient population.
Like we don't see a drastic drop-off, um, and or we don't see an increase.
So we don't see people calling 911 more often because they're an EMSA care member, and it would be easier than going to an urgent care.
We want to make sure that people are getting the right care that they need, but in no way are we discouraging them from calling from calling 911.
So at the end of the two-year moratorium, number one, we look at our our transport and um uh run data monthly.
So we will be able to catch very early on if something is going on in any one of that uh in any one of those buckets of our patient population.
Our two-year moratorium, uh, as long as it goes as expected, then the treatment in place fee will um you know will be uh we'll begin to bill those to patients.
And then Sonia, do you want to talk about what we expect from?
Yes, um, so we will bill those to patients at that time, and just like we have proposed if they are uninsured, they will also receive a 40% um reduction in that fee as well.
Um today, if you receive health care services from any other health care entities, we do not expect for those charges to not show up.
And so it's just really aligning our services with the rest of the health care industry, where if you receive services, then you expect to be charged for it.
We're hoping that a lot more people will sign up for EMSA care and see the value at that EMSA care is because if they are EMSA care members, even if they're uninsured, then they will not have to pay out of pocket for treatment in place in two years' time when we roll it out.
And we won't retroactively bill any uninsured patients once the two-year period ends.
There's not going to be any bills that come out from something that happened in January of 27.
And what does it look like with your bilingual providers for EMSA?
Do we have so we do uh we do have some bilingual providers, but unfortunately, um the way that you know our system our our goal is to get the the most appropriate care to you quickly?
So if we happen to have a bilingual provider on unit 142, um, but the closest ambulance is unit you know 147.
We're gonna send unit for 147.
We do have a variety of translation services available to our patients and our providers in the form of the language line, which is what the city of Tulsa's 911 summit uses, and then we also have our community uh engagement manager who sits in the creator Tulsa area Hispanic Latinx and Bears Commission.
We will be creating uh Spanish language documents as we um sort of do the MSegare open enrollment that would coincide with the implementation of this um so we do have uh a two pong approach to reach that.
We've done the bilingual MSEC care ads for eight years, and we have several Spanish language resources on our website.
Okay, and then one uh final question the 32 percent increase in wage and compensation.
When was the last time there was an increase in wage and compensation?
Uh last July.
Last July, and so we're we're requesting a 32% on top of that.
No, that 32% is our increase in wage and compensation um over the last four years.
So basically um our it's it's just another avenue.
Our wage and compensation budget is um one of our highest line items, and so as we are, you know, we're just showing you the increases in our cost to operate your EMS service.
Do you see the little asterisk on our handout?
It's not well, I don't that slide's not even up that we're talking about number eight.
It's 2020 to 2025, 32 percent over those five years.
Yeah, so yeah, yeah, still I think the public would like to go.
Sure, of course.
Council Dr.
Red.
Thank you.
Um as we know, post-pandemic, these uh frontline health care worker jobs are hard to fulfill and sustain because it's the whole world got real nasty about that.
I mean, I don't know about you, but when I pick up my prescription at Walgreens, I have like a warning about you better be nice to our pharmacist, and you know, yeah, healthcare providers are literally being violently attacked, and we've seen incidents of ambulance opervers getting punched through the window and things.
So um I have questions, which I'm sure will be no surprise that they're coming for me on this, but I'm just for our friends in the room, their friends at home as we're having this conversation, and did with EMSA's change in the Eastern Division with beneficiary and non-beneficiaries um cities, has that like is the volume remain the same, and is any of this cost adjustment revenue um enhancement adjustment related to service area changes for our division?
So I'm happy to answer that.
Um the actual the the truth is we've actually seen an increase in uh in transport volume in Tulsa.
While we have lost non-beneficiaries, so again, the city of Tulsa and the city of Oklahoma City are the only members of the EMSA trust.
We have lost non-beneficiary members.
Um we have seen uh so the way that it it is budgeted is they're only charged for their patient population in terms of what their piece of the EMSA budget is.
So none of this is related to that.
Again, we have quickly um and in honestly, unfortunately absorbed any volume in Tolls of the City of Tulsa proper for the non-beneficiaries.
And I say unfortunately, because what that means is our residents are using 911 a little more often, and then we've also seen pay duration growth because of the non-beneficiaries that he's leaving the trust, our residents are using the city.
No, I just mean so we try to fall tracking.
Sorry, we have quickly absorbed any loss of volume from the we're making the difference.
And do we anticipate um so let me just reflect back to you what I heard when non-beneficious fishary cities left, you just adjusted operations according, like the outline of where you were serving shrunk, but the number of people that are using the services didn't necessarily.
But there was a loss in revenue when those non-beneficiary cities stepped away, or no.
I mean, sure, briefly.
Um, and if we I guess you could say, you know, I'll take the city of of uh sand springs.
Sure.
So let's say that their patient population was 5,000, right?
I mean, obviously, um, depending upon their payer mix, we would be generating revenue and sell capacity for those 5,000 residents.
Um, what you know, our operation model didn't change.
So what we did is then take those resources and redirect them back to the city of Tulsa proper.
Um we didn't have stationary posts out there, uh those were always outlined.
Okay.
Um, and so um so sure, there you could say that those 5,000 calls, um, you know, we could have seen a slight decrease in revenue.
Unfortunately, we have quickly seen that picked up those 5,000 in the city limits.
Okay.
Um, as we know, our systems designed for TFD to respond to certain priority calls.
So if TFD as designed gets us gets to the patient first, MSA's on route and getting there, and the patient refuses this transport.
Can you talk about how this treatment in place would be handled?
Who gets billed or does anyone get billed?
Yeah.
So um, so primarily uh if the system is working as operated, then uh Tulsa Fire, uh, our Tulsa first response partners are going to respond on our highest acuity patients.
The majority of those should be transports.
So just because of the prioritization, but let's say for some reason not, um it depends.
If Tulsa Fire responds, gets there first, does an intervention, we do not bill for interventions done for other people, and so only if care is handed over and we do an assessment and an intervention, would a uh resident get a bill for treatment.
Okay, okay, and TFD is not billing for treatment in place that I'm aware of, so just throwing that out there.
Sometimes people Tulsi Fire doesn't they don't pay for anything for anything, they they're funded out of general funds.
That's right, and then uh a small portion out of MSEC care.
Right.
We do that reimbursement.
We made an adjustment a couple years ago on supplies, and then we do one-for-one pharmaceutical and supply uh on scene.
Yeah, um, so the final thing, because we did make an adjustment on some insurance billing related to hazmat services that fire does perform, and then we got a little bit of concerns elevated back at us about what that just premiums, and so that's my final question.
Is like um if EMS agencies across our state start billing for this treatment in place, because that those claims eventually cause the insurance companies to adjust those premiums for people that are privately insured.
We do not anticipate that to happen.
Um, other things that have implemented treatment in place we have not seen, or they have not seen an increase in premiums and um premiums are unrelated to the cost of ambulance services, they're typically aggregated to the group, uh depending on if it's an employer sponsored or state sponsored, it's really based on the health the total health care spend of which ambulance is a very minute part of that.
Um we've seen premiums increase for so many as I've never had an ambulance um transport, Malcolm would but my premiums have increased air over year over year.
Sure.
So we do not anticipate for that for treatment in place to then cause uh an increase in premiums across insurance providers.
I'm just wondering a little bit, I mean, this is just me thinking out loud to policymakers.
Thank you for mentioning that there's some moving bills down at the state that could impact one way or another our constituents around health care.
Um we know that a larger segment of Oklahoma's including Tolson's are using emergency calls as like rather than prevention or even like clinic minute clinics, whatever.
So I would like on the two-year tracking if we can look at some data that says like more people are doing the treatment in place, refusing the ride, but getting, you know, the thing that maybe they would have gone to urgent care for.
Um just curious.
Yeah, they're all I think correct me if I'm wrong, but the TFD hazmat would be uh automobile or insurance.
I was just referencing to my colleagues that we made another uh policy decision that it was like we're leaving money on the table.
Yeah, companies would reimburse for this if we could find a way to bill for it.
So we hired third party, we were like, okay, because we also had a a directive to all these departments to find revenue and contain costs, which is what we do.
And so that's what they did, and then community members came to us and said this is going to impact premium.
So I wanted to learn from those decisions and make sure we were doing an if-then model here for us on the decision making treatment.
Um I think the two-year thing that you're gonna do.
Yeah, I just think that'll be helpful.
Since you're designing the tracking, if we can just also you know, see like can we look and see?
And I don't know what kind of surveying happens in the field, like are you refusing today because of concerns about pay or what?
I just don't know.
Yeah, so um our goal in the field is patient care quality patients.
So we do not ask our providers to collect insurance information when we dispatch, we do not know if you have insurance, if you're uninsured, if you're underinsured, we handle all of that on the back end because we'd want our providers to focus solely on the patient.
But on the back end, do you get that information insured, uninsured?
I mean, when I was in my 20s and would get like an offender vendor or whatever, and they would be like, Do you know, do you want to transfer?
It was like I was already doing the if then what is my bill gonna be, and do I really like do I really need an ambulance ride?
You're sitting in the middle of the freeway in shock trying to make these decisions.
So I know myself when I was on a limited income, I definitely was running those scenarios and doing things like I'll just take myself or whatever.
So I know it's on people's minds.
I think the big takeaway here for us, aside from you know, having to vote on these things, and Oklahoma City already voted, right?
No, so Oklahoma City uh will vote.
Uh this goes on the open city um council agenda on May the 19th, so we have some time here to engage with constituents.
For those of us that have town halls regularly or even just our social media or whatever, you know, we have someone in code enforcement that specifically looks at the multifamily and does an assessment as to whether or not they're as a property ownership group and enrolled in MSICare.
If they're not individuals can enroll on their own, but I still think that needs more amplification from us.
So at town halls and things, if we can have those flyers and those um descriptions of how people can if they're all bills paid or whatever their situation is, they can still do this six dollars a month or what it's a one-time fee, Adam.
Like $80 a year or something.
We have purposely set the implementation date as October 1st, which is uh after the city of Tulsa's open enrollment month in August, and the city of Oklahoma City's enrollment month in September.
We are going to do about a two and a half times larger um engagement campaign, and a lot of that um you know we'll be focused on explaining how people check if they're enrolled or not, and then if they're not enrolled, how they go about doing that.
You're exactly correct with code enforcement multifamily housing, it does get you know, it's a it's a little more muddled than the single family.
Um, but landlords are required to give their tenant a waiver that acknowledges that the tenant understands that facility or that property is opted out of MSicare, and here's how they can join independently.
And does MSICAR go with the actress of the residence or the person in the residence?
So it for the city it's with the utility accounts which are tied to single family homes, but the um direct subscriber is for a year, and it's for the person.
For the person, okay and it's $65, which is the $545 monthly fee times 12.
You can actually join that at any time during the year.
It's just um not prorated.
Okay.
Um, but we will be doing uh a robust public engagement campaign, um, including some town halls and direct mailers to landlords explaining what's happening and how they can and I think as we've learned uh 50% of Tolsons are renting, and we know our communities.
I think it's important that we just make it part of what we share with communities because it can be confusing if you don't if you didn't grow up here or you don't, you know, you're in transplant, it's all of a sudden like what is this?
And um I think more often than not, I'm probably you can share anecdotes.
Uh people discovered like I should have been paying the six dollars a month or five eighty-five once they get that first bill for a ride, and then it's like you know, little buyers or more.
So um yeah, and we are I mean, I've been to several of the town halls and events that counselors put together.
We are happy to explain MSicare and how to sign up.
Um, and like I said, we're gonna be doing a much more robust campaign because there are some changes that we want to make sure um that our residents are aware of.
Anything else?
Okay, counselor Lakeland.
I just on MSecure.
How many of our residents?
72%.
It's like 70.7% of single family households are enrolled.
There are two opportunities that month of August, and then at the start of service.
Um so you know, just make it we've worked with uh customer care center to make sure that the scripting and language accurately tells the person setting up service what's included.
Um but also if you know 45 days later you're like, wow, I should have signed up for that, you still can directly with us.
Yeah, um, but we have no update and you know we have no intentions of of changing anything with the MSICAR marketing.
We still want to talk about the benefits, but we um we definitely want to make it a little bit more visible about what's changing because we think that the treatment in place aspect is uh is gonna be a huge map of member benefits.
It's just it's so beneficial, and you you don't you're not really affected um by this change if you have MSecure.
So that's at all.
You wouldn't know yeah, and we're not trying to sell more MSC care memberships.
I mean it's not like a membership anyway, but there are those benefits, and you don't have to worry about it if you do have an accident on a freeway and you're 23 or whatever example that you use, counselor director right.
Um it's it's just taken care of.
You get the care that you need, and everybody else takes care of everything else from that 44.
Okay, that's all wonderful.
Anything else from anyone?
All right, well, thank you all for being at the table.
Thank you for your time, council.
Thank you.
Thank you.
All right.
Uh final agenda item.
Well, number six.
Uh travel authorization for council rules and order of business.
He's the estimated amount of $1,550 for counselor Hall Harper to travel to Omaha, Nebraska to attend the 19th annual rebuilding the village conference and revive Black Business Expo to be held May 5th through the 8th, 2026.
This is for her flight, hotel, and for DM.
And uh Sarah, will you share about this?
Or uh yes, the counselor Paul Harper can tell you more about the event, but so your council rules require that if your um annual travel exceeds $500, then it needs to be approved by council, and we put it on the committee agenda.
Um, and so there are sufficient um funds in the travel account for uh the counselor to attend this event.
Um, and then we did just put a note on there that um there was a a flight credit, so it actually won't be quite at that $1,500 level for this event.
Is it with spirit?
What no, no, no, no, it wasn't temporary house for it's better who it's with.
I am so sorry.
Flight credits, flight credits or southwest.
You should have five years.
Anyone else?
Uh speak about this.
Uh counselor Hall Harper, do you want to speak about the conference call or go over you?
Very good.
I highly recommend I went one year.
It's very dynamic and inspiring, and I think that organization is putting like an outpost in Tulsa and doing some work here.
We're duplicating.
No, I'm not sure.
Like bring their um click.
Maybe I'm I'm misspeaking about it, but yeah, the environment network, we're duplicating it model here.
Oh, and so that's a model that got national attention.
If you've never gone to that conference, it's pretty amazing.
So definitely interested for sure.
Well, thank you all uh for coming today and joining us online.
Um last order of business, we are adjourned.
Because any time water is turned off, there is a chance your system will lose some pressure and you.
Tulsa City Council Urban and Economic Development Committee Meeting - April 22, 2026
The committee convened on April 22, 2026, to discuss five agenda items: a new increment district at Tulsa International Airport, the annual assessment roll renewal for the Kendall Whittier improvement district, an affordable housing trust fund allocation (later tabled), a presentation from EMSA on rate alignment and treatment in place proposals, and a travel authorization for a councilor. The meeting proceeded with staff presentations and councilor questions, but no formal votes were taken; items are expected to appear on future council agendas.
Consent Calendar
- No items were designated as consent calendar.
Public Comments & Testimony
- No public comments were made during the meeting.
Discussion Items
-
Tulsa International Airport Increment District E (TIFF District 26): Airport staff (Alex and Jeff) presented a request to trigger the fifth and final TIFF district within the airport’s project plan. The district covers approximately 1,500 acres and includes the Agile Space Industries group, which had a groundbreaking earlier in 2026. The district is a combined property tax and sales tax generation district to fund future airport development. The statutory deadline for activation is June 16, 2026. Councilors expressed support for the airport’s work and the Alaska Air addition.
-
Kendyll Whittier Improvement District Annual Assessment Roll: Samantha from the planning office presented the renewal of the assessment roll for the district, which is in its sunset year (ending June 2027). Changes include one property address change and three properties rezoned from commercial to residential (exempt from assessment), reducing the annual budget by $1,030.11. The total annual assessment is now $47,604.31. Funding supports landscaping, trash removal, security, beautification, lighting, parking lot repairs, and administration. The resolution sets a public hearing for June 10, 2026.
-
Affordable Housing Trust Fund Allocation (Item 4): The item was tabled after Councilor Gilbert (District 5) expressed that he had not been informed about the project, which involves the Oyo Hotel and 147 affordable housing units. The item was moved to the next committee meeting to ensure full council awareness.
-
EMSA Rate Alignment and Treatment in Place Proposals: EMSA representatives (Johnny Easy, Jenna, and others) presented two proposals for council consideration: (1) updating base transport rates for the first time since 2012, bifurcating rates by level of care, and (2) implementing a treatment in place fee of $500. They emphasized that this is not a request to increase EMSAcare rates, but rather to maximize third-party revenue and preserve Fund 121 for system sustainability. Key elements include:
- Rate alignment could bring in an additional $1.9 million in revenue.
- Treatment in place fee could generate an additional $1.6 million.
- A 40% uninsured discount will be implemented to offset impacts on uninsured patients.
- A two-year moratorium on billing uninsured patients for treatment in place to gather utilization data.
- EMSAcare members will see no change in out-of-pocket costs.
- The proposals are designed to reflect the actual cost of care and align with industry practices. Councilors asked clarifying questions about billing practices, impact on uninsured and Medicaid, bilingual services, and the two-year tracking. The proposals are expected to be on the council agenda in May.
-
Travel Authorization for Councilor Hall Harper: A resolution authorizing travel to Omaha, Nebraska, for the 19th Annual Rebuilding the Village Conference and Revive Black Business Expo, May 5–8, 2026, with an estimated cost of $1,550 (reduced by a flight credit). Councilor Hall Harper spoke briefly about the conference. The item was approved by committee.
Key Outcomes
- TIFF District: No formal vote; staff will proceed to bring the ordinance to the full council before the June 16 deadline.
- Kendyll Whittier Assessment Roll: The resolution was directed to be filed with the city clerk; public hearing set for June 10, 2026.
- Affordable Housing Trust Fund Allocation: Tabled to next committee meeting.
- EMSA Proposals: Discussion only; the proposals will be placed on the council agenda for May 2026. Councilors requested data on tracking treatment in place impacts over the two-year moratorium.
- Travel Authorization: Approved by committee.
Meeting Transcript
How quiet everybody is. We're live. All right, good morning, everybody. It's 10 30 in the morning, April 22nd, and this is the Tulsa City Council Urban and Economic Development Committee meeting. My name's Anthony Archie from Council District number two. First item of business is to call this meeting to order. Second order of business. The ordinance naming increment district E of the amended and restated Tulsa International Airport Economic Uh Development Plan as Incentive District Number 26. City of Tulsa and establishing the date for the creation thereof, ratifying and confirming the actions recommendations and findings of review committee and the Tulsa Metropolitan Area Planning Commission with regard to increment district E ratifying and confirming the action of the City of Tulsa in enacting ordinance number 23475. I need to continue on, probably. Sarah's not here. I'll keep on reading. No, it's fine. Okay. No, yes. You stop wherever you have to do that. Okay, you just have to summarize what's there. Great. You don't even have to read it. We're adding to the um to the plan. Okay, so Alex and Jeff are here with us. Thank you for being here. Good morning. Thank you for having us. So we are officially requesting permission to trigger our fifth and final TIFF district, which is within our project plan. Um it's exciting to be able to trigger it because we already have a company that is starting to develop the Agile Space Industries group groundbreaking that we had earlier this year is within this district. And so this is a combined property tax and sales tax generation district. So as they start construction on that, any um taxes they paid, we can partner with the state in order to receive some of those funds back and use those funds for future airport development. But it's about 1500 acres, right, Jeff? Yep. Um of our about 4900 acres that we have at Tulsa International. Well any questions. How many acres? 1500. Yeah. 49. Great. Well, thank you for the work that you're all doing. Let's expand the tip. Okay. I have something real quick. Oh, please. Thank you for all your hard work out there at the airport. Really do appreciate it, but thank you for bringing Alaska Air. You're doing really well. So fine. Yeah. Sure. Jeff, did you want to say anything? No, I just the statutory deadline for activating this TIFF is June 16th.
openpublica.com