0:01Revenue forecasting commission will now come to order.
0:04I will now call the role.
0:09Commissioner Merriman.
0:11Chair Anthony, you have a quorum.
0:14Good evening, everyone.
0:16This is a particular particularly special IRC meeting as it does mark my last one as CFO.
0:22It has been an honor presiding over these meetings.
0:24And I thank all of you for your professionalism, hard work, and devotion to the independent revenue forecasting commission.
0:32Since we last met, the team has been analyzing the various factors driving lower revenue growth.
0:38And we will delve into those specifics very shortly.
0:41We are working very closely with the Cook County Health Team, monitoring and adjusting our long-term forecasting assumptions as additional OLBA information becomes available.
0:52The county is looking ahead to fiscal year 2027.
0:56And so with that, we've collaborated and conducted outreach with multiple departments to gather data to inform our near-term revenue estimates and preliminary forecast schedule to be released in June.
1:08Lastly, that's lastly, I wish to convey my appreciation to my amazing team and the outstanding commissioners for the hard work that each IRFC meeting requires.
1:20And without further ado, let's review the agenda and get this meeting underway.
1:25The first item on the agenda is the approval of the minutes from the meeting of January 28th, 2026.
1:32Chair, we will need a motion to approve the minutes to proceed.
1:35Is there a motion to approve the minutes?
1:41So it's been moved by Commissioner Merriman, seconded by Commissioner Dabula.
1:46All those in favor signify by saying aye.
1:49All of those polls signify by saying no.
1:52In the opinion of the chair, the ayes have it.
1:54The meeting minutes will be filed with the council Cook County Secretary of the Board.
1:58The next meet the next item on the agenda is a staff presentation on the quarterly updates and the long-term forecast.
2:04Lancy, if you could please proceed.
2:07We'll start with quarterly updates.
2:16You know, in particular, we've been in close collaboration with Cook County Health staff as there's been a lot of different uh changes uh that we are considering how we might integrate forecast as we uh start rolling into next year when we will have more provisions of OBA take effect.
2:42Uh so the three deliverables from the recommendations report from last August.
2:49Uh first one revenue growth.
2:52I'm gonna hold off on talking about that till the next slide.
2:55Uh assessing the impact of OBA on the health enterprise fund.
3:00Uh one of the things that we did this quarter was we reviewed the state's proposed 2027 budget to see if uh really if they were uh anticipating any impacts uh fiscally that were different from what they'd shared before.
3:15And then lastly, for ARPA, we are continuing that sustainability analysis and in particular right now we are looking at developing an allocation strategy for the reserve.
3:27So we have 158 million dollars in reserve that we intend to use over four years to sustain uh a set of those ARPA programs, and uh we are determin we are working on determining how we're gonna allocate that across these programs.
3:45And then quick update though on that first item, the project where we are looking at some of these drivers of low revenue growth and uh assessing and evaluating strategies to mitigate those.
4:00So we've taken a look at our revenues and we've come to some are basically some findings that we've arrived at with respect to our uh low revenue growth for certain sources.
4:16So first item, we have the county has many fees and also volume-based taxes.
4:23So when I say volume-based taxes, I mean uh it's like uh gas taxes per gallon, alcohol tax is also based on volume, and cigarette, other tobacco, these are all based on volume and not price.
4:38And so these rates haven't increased at all in recent years, and that means that these tax revenues would only grow if uh the actual consumption of these items were to grow.
4:52And then second item, inconveniently, the larger consumption and demographic trends for many of these same taxes mean that they're not growing.
5:03So you're seeing a situation where gas, alcoholic beverage, cigarettes, uh, these are all taxes where consumption you're we're not seeing them grow substantially, and we're not expecting them to.
5:13And so that means that we're seeing flat or even declining revenues uh in our forecast for these items.
5:20And then this even applies to you know, things like off-track betting, the uh taxes we get from those facilities and cremation fees, even so these are uh items that we've looked at.
5:32We've also uh looked at our property tax levy, our property tax levy, which is uh set annually.
5:39This base levy has not increased.
5:42The base levy hasn't increased in about 30 years, and then since 2012, we've been having basically an incremental increase in the levy to account for new property and also TIFF and incentive properties coming back online, and so therefore these levies have not kept up with inflation.
6:01And then lastly, policies at the state level impact our revenue.
6:07So we've talked about this in this meeting many times PPRT.
6:11Uh we've seen a situation where changes in what the state is doing, whether that's reallocating uh PPRT revenue to other funds based off of true up adjustments it has to make, and that results in declines in our PPRT revenue, cannabis tax.
6:32Uh that's a situation where policies at the state level impacting the overall level of taxes imposed, dispensary licensing, that all has impacted our expected revenues, and then even sheriff fees, legislation that was approved last year regarding private process servers impacted those revenues significantly.
6:53So uh that's where we're that we're at we're at on our findings, and we are currently looking at uh different strategies that might help mitigate some of these challenges.
7:11Um I I don't actually think I've ever seen data about the distribution of tax revenues over time.
7:19Um maybe we could get that data.
7:24I'd just be interested.
7:25I know that that the revenue sources, although there's a bunch of them, they they aren't that big, but I just wonder a little bit about how much uh their stagnation has mattered in the overall picture of things.
7:41Um and then the second question I have.
7:45So this information, I I did quite a bit of work on cigarette taxes earlier in my career.
7:49And what you know, there is like uh the World Bank and or the World Health Organization, other groups will very much say, yeah, the taxes on cigarettes should be a share of the price, so it should go up naturally with inflation.
8:02I don't do we have the legal right to do that.
8:05I you know, I'd have to double check specifically for cigarette taxes, but I know like a lot of our taxes, the state statute requires us to do volume-based for terms of whether or not that's cigarette.
8:19I'm not sure I have an answer to it at this moment.
8:22I don't know if uh yeah, if Tina, Tina might know specifically for if that the county's code, if that part of the county's code applies to cigarettes or not.
8:33That's an interesting, it's an interesting if the if the tax is also kind of expect is intended to kind of uh incentivize less than then you yeah, and theoretically uh it would need to keep up with the price to do it to do that piece of its job.
8:53So yeah, that's certainly like best practices sort of suggest that's what you should do.
9:01Yeah, well, we'll uh is there something you can apply on now.
9:08I mean, I know that we are mandated or based on the state code, we it has to be um like a it's not based on the price.
9:17It's we have to charge like based on volume, so it's per cigarette.
9:23Um yeah, like Lindsay said it's definitely designed, I think.
9:28So we're trying to discourage smoking, even though obviously we like the revenue, but okay.
9:43But we could look into anything, you know.
9:46We need to look into further.
9:57I'll pass it to Michael for the general fund forecast.
10:01Um so let's get going on the general fund long-term forecast.
10:06The first slide it's uh economic indicators.
10:08Uh we'll just quickly review as these impact on any of our projections.
10:12On the left side, the inflation is up to 2.3% for March.
10:18It is projected to be 3.1% in April, and then the projections were to decline uh steadily over into the out years.
10:25On the right side, you see the GDP forecast.
10:28Um projection for 26 and most of the uh most of the predictions are that it should decline in 2027.
10:36Although Wall Street Journal is an exception, that will go up, but they're starting from a lower point in their projection.
10:43Um the Wall Street Journal projects a survey, as is the service professional forecasters.
10:50Um but again, just quickly review as these impact our projections.
10:54There's no questions, uh, we can move on to the next slide.
10:58So the largest revenue source in the general fund is sales tax.
11:02Um, and so you see on this chart uh the sales tax for this year, the yellow line is the actual sales tax revenues YTD compared to the budget, which is the blue bars.
11:13That's our budget for this fiscal year.
11:14Uh, Y2D we are higher by 7.7% uh or 44.9 million year to date.
11:22Um based on the actual uh the actual hit the actuals that we have through these first five months.
11:30We have made adjustments going forward um to the variables used to account for legislative changes and the increased actuals also impact regressions.
11:38So uh we'll see on later slides how this impacts progressions.
11:48Okay, so slide 10 uh showing what we've changed in the FY26 revenue projections from the forecast that you saw last January.
11:57Uh on the left side is the previous forecast.
12:00Uh on the second bar is the increases of 246 million uh for various line items, a few line items decreased, totaling 24 million, and then on the right side you see uh the new revised forecast of 2.9 billion.
12:15And uh the next slide dance, just really the same information but in the data format, so it's uh easier to uh glean information.
12:24This is a breakout of that 222.3 million increase for FY26.
12:30If you look at the FY26 column, we see that totals uh 22.3.
12:35The largest increase for FY26 is a cigarette tax increase from our projection in January.
12:40That's due to a settlement uh that came in of uh 115 million dollars.
12:46So that's why that is uh shows such a large increase.
12:50Um the next largest item is uh sales tax again.
12:56As I mentioned earlier, 44.9 million for the first five months uh was the difference from the budget to the actual, and then an additional 42 million increase for the last seven months for the fiscal year based on uh again the increase that we have in actuals and our variable adjustments uh causing it causing it the regression to show an increase for the last few months of the year.
13:24Um other increases are uh just to know are the investment income increase due to a change in fiscal policy, which puts more uh investment income into the general fund instead of certain other funds.
13:37Um and uh also see the increases in the out years.
13:41Uh the total increase, like we said is 222 million for FY26 for FY27 to 30, that totals 455 million increase for a total for the five-year period of an increase in 677 million in um in revenue projections.
13:59And if there's any questions on other specific line items, we could try to address now, or we don't have the information in front of us.
14:05We could always get back to you later.
14:07Or we could move on to the next slide.
14:15Okay, so this slide is the F surplus or deficit projections uh for the past few years and the projections for the future years.
14:25Uh this is also known as the alligator chart.
14:29Uh, this chart as well as the comparison chart on the previous slides, exclude the transportation fund, while previous versions last quarter uh had the transportation fund.
14:40It is important to note that the unfavorable general fund net results in the forecast starting in fiscal year 27 are primarily attributable to expenditures not being allocated to transportation fund revenues due to a court ruling in January.
14:55The favorable number for FY26 is driven by the cigarette settlement and sales tax increase.
15:01For the out years, uh expenses are projected to increase faster than revenue, contributing to increasing deficits, uh, which will have to be handled on a policy side.
15:12Um just as a note, the jump in expenses you see from FY24 to 25 is due to a removal of the negative expense having to do with the transportation fund as mentioned earlier, due to the court ruling in January.
15:32Uh we can move on to the next slide slide, which shows the uh unassigned ending fund balance, um, which you see is uh decreasing as the years go on.
15:42This is this is really driven by the previous slide.
15:44The previous slide showed uh increasing deficits each year, and that contributes to uh it increasing uh uh increasing problems in the unassigned uh fund balance.
15:58Again, this will be dealt with uh by increasing revenues and/or decreasing expenses on a policy side.
16:05So yeah, I'd like I'd like to just say this is uh probably the most uh impactful or most important slide in the presentation, and then uh you know, I've been on this commission for a number of years.
16:21I've never we've always looked, this is this slide has always looked good.
16:26This is you know uh a real something that really needs to be emphasized as uh a problem that has to be addressed.
16:36Uh so I just want to make sure that everyone's fully aware of it and uh should be brought to the attention, certainly of uh elected officials that uh there needs to be adjustment.
16:49And I also want to say I I neglected to say earlier that I want to thank Tanya so much for the work she's done on this commission, and we will miss you.
16:59Appreciate your work here.
17:02And thank you for your comment.
17:04Um when we look at slide spectrum.
17:09When we look at slide 12, actually 12, which drives slide 13.
17:14I we're gonna have to pass a balanced budget.
17:17And so as um as Michael mentioned, is it's gonna be having to raise revenue or decrease expenses so that we can pass a balanced budget.
17:28It is going to be incumbent upon our team when we look at our fund balance to really stay on top of the policies that we've established on how we use the fund balance.
17:40And so when we start to address slide 11 on slide 12, then we'll start to see a better uh more positive impact on slide 13, provided that we stick to our policies and not just try to plug these gaps that we see with our fund balance.
17:57Um, so you know, so far our the team that we have, the commissioners that we have have been in alignment with our policies and procedures, and it's really going to be incumbent upon this team to continue to enforce that.
18:13Yeah, I'd like to just reiterate what David said that was sometime to me and our at the presentation that we have monthly.
18:24Yeah, so I I think that it's really great.
18:28I'm sure you're talking to people.
18:29The discussion, you know, should start now and not wait until October or whatever.
18:36And um, that discussion should also understand where this came from because this was a part of a decision that we we made years ago, I think, with uh with the constitutional amendment, and people should understand that.
18:54I think what amendment?
18:57The amendment which required all transportation funds be spent for transportation, and then the subsequent court decisions about coming out of that.
19:08So I think it's important to understand that this is not about lack of foresight in terms of having a balance between spending and revenue.
19:26It is very concerning.
19:29Thank you for uh just highlighting that.
19:31Appreciate your support on anything that they come up with.
19:41So uh this slide shows the revenue scenarios, uh, the baseline is what we've been talking about.
19:46That is the gray line.
19:48Uh and it just shows what the revenue scenarios would be with an optimistic or a conservative uh scenarios.
19:54Again, these are based on Moody's analytics from their March report, um, their assumptions, uh optimistic baseline concerns.
20:00Their assumptions optimistic baseline concerns.
20:03Some of the bullets that Juice is using, and we're using their information to show how revenues would change based on each of those based on their assumptions.
20:24So this shows that the growth metropolitan product and the unemployment rates that are used in the three different scenarios that we're charting.
20:34So again, just you could see on the right side, just for example, the conservative scenario shows a large increase in unemployment in 26, 27, and 28 before falling, uh, which is not seen.
20:49And on the left side, you can see again a decrease in gross metropolitan metropolitan product of that.
20:54So the previous slide just showed how those items on this slide would drive our revenues.
21:00Then slide 16 uh is really a repeat of slide 13 with the fund balance.
21:07Uh we already saw what the what the baseline scenario is in those gray bars.
21:11And then again, if we had the conservative or the optimistic scenarios, uh, how that would uh change the unassigned ending fund balance again, the magnitude of the impact to our revenues uh these different scenarios is not so great.
21:27So uh Michael, I just want to make sure we have the timing here because uh I think when we talked uh last week, uh you hadn't gotten the most recent projections and to what extent do these current situation and uh do you have a sense of how what the magnitude might be once we those are incorporated.
21:53I mean, so when we when we did speak last week, uh it was based on a February Moody's uh display on the March Moody's release.
22:01So uh whatever whatever changed from February to March, which is again the banks is not that much.
22:06If you go to the if you go to one more slide that you could uh sorry, this one you can just see the assumptions and uh you know how the different optimistic versus conservative versus baseline scenarios assume.
22:20And again, the team just you know pulls a few different bullet points uh from Moody's from Moody's report, but we could we could get you more more detailed assumptions uh based on you know different the war and the oil prices and whatever else is going on.
22:36Uh, we could get you a list of those assumptions that were used if you'd like.
22:41I mean it, but I think even more just you know, we're now we're almost at the end of April.
22:46Things do change very fast.
22:47We just don't, it's there's a lot of uncertainty up there.
22:50A lot of them certainly, a lot of volatility conditions.
22:52I mean, I think the current administration just um, you know, it causes I don't say cost the current administration due to the administration, there is a lot of uncertainty and volatility, and that is to be expected.
23:06So to your point, the fact that it's now April, we're using a March forecast, but uh you know who knows what's gonna happen in May.
23:20Um, if there's no more questions on the general fund, you may speak about the health fund.
23:27All right, thanks, Michael.
23:31All right, so uh yes, so here we have a snapshot of the uh baseline uh forecast for the uh health fund revenue and expenditures.
23:42So in our previous uh estimate that we presented in January, um, just looking at 2025 really quick.
23:51We were at that time projecting 2025 to uh finish with the surplus, about 166 million.
24:00Uh as you can see here, it changed uh you know, just the smidge uh just under 165 million.
24:06Um, so that's uh what we're looking at right now for the health fund as far as closing out 20 fiscal year 2025.
24:14Um looking at the current fiscal year, uh so for 2026, um, a notable change from the previous forecast, uh, is that we're now estimating there to be a deficit of about 41 million or 42 million dollars.
24:29Um, this is down a bit.
24:31Um in January, we are estimating that to be um uh about a hundred million dollars uh in deficit.
24:39So that's come down quite a bit.
24:40Uh and this is mostly driven by updates on county care side, which I'll touch on some of the upcoming slides here.
25:00Uh and then lastly, just looking ahead of 2027 and into the out years, uh, you know, similar picture that we've been seeing in the last couple meetings where we're anticipating uh growing deficits into the out years, um primarily because of the anticipated impacts from uh OBA on uh CCH side.
25:13Um and so before I get into some of the factors uh shaping the forecast on the next slide here in the presentation.
25:20I'm just gonna walk through a few uh policy updates.
25:25Um recent uh the county um so there are two new policies that were created as part of the uh fiscal year 2026 uh budget resolution that we wanted to cover uh as they do relate to the health fund and uh specifically uh impacting health plan services.
25:45So the first polished policy here is the establishment of a uh working cash balance for health plan services, uh just to ensure that uh county care health plan services has adequate uh liquidity uh to be able to provide uh uninterrupted services, uh, be able to um uh cover managed care claimed expenses that may arise uh that revenues um uh can't maybe cover.
26:12So um the working cash balance uh something that will be estimated uh each year.
26:19Uh it's going to be equivalent to about one and a half months um of expenses from the most recent uh CCH audit.
26:29Uh so for example, for the fiscal year 2026 working cash balance, that was estimated to be about 393 million.
26:38Uh and so that was based on the 2024 uh audited claims expenses for CCH was which was the most available at the time.
26:49And so this uh second policy established was part of the 2026 budget budget resolution is that the county uh is going to maintain a cash reserve for managed care claims.
27:01Uh and so this is just to help support managed care claims again.
27:05Yeah, if revenues received in the current fiscal year are not sufficient enough to pay down claims.
27:12Um and so uh this is not a new or like a separate fund.
27:17Uh this is essentially just any cash exceeding the established working cash balance, which I just mentioned, um any available cash exceeding that amount will be eligible for this purpose.
27:28Uh and so as part of the budget resolution, the the county's budget director uh is authorized to be able to make uh you know a continuing appropriation to deploy this such cash to pay down uh unanticipated um uh rises in claims.
27:46And so now just circling back to the forecast.
27:50So, due to the high intensity of uh utilization at the end of 2025 uh on the health plan services side, uh the county did make uh a continuum appropriation in the first um using this cash reserve in order to pay down um the anticipated um rise of the managed care claim expenses.
28:14So I'll pause for any any questions since oh yeah, this is I think the first time at least I've seen this.
28:20I very much appreciate you putting this information in.
28:22I I guess I wonder about a few things.
28:24Um is why uh is there some industry standard about this?
28:31Do you know why one and a half months was chosen as the goal?
28:36Um sure about one and a half.
28:38You know, the I think the one and a half months was really I'm not something where we were we had a discussion with Health Line Services about what would kind of make sense for their operations, and you know, I don't know.
28:51Yeah, but in addition, I mean, I think you kind of think of the two months as being the kind of value that you would want to carry for them.
29:00Um I think that's consistent with what we've been asked to provide by uh oh, what's the name?
29:07Uh the Illinois Department of Health Human Services had requested that the a couple of years back that the that the healthcare services maintain a reserve of about two months.
29:18Obviously, the county is still responsible and accountable for the operations of the health care system.
29:24So uh regardless of the amount that um you know the two month kind of value, I we thought it was appropriate to kind of cap it at one and a half, um, with the understanding that we would still be accountable for any leverages above and beyond that.
29:39Okay, okay, I appreciate that.
29:44Um I guess I'm not sure I understand the managed care claims cash reserves.
30:04So the HPS that could go for the hospital system or for the managed care.
30:09Is that kind of the idea?
30:11Or what like how do these two things interact?
30:14I guess it's for managed care specifically.
30:18Yeah, it's yeah, and it's in in their specific cash.
30:24The HP, the managed care claims reserves are but the working cash balance is for both.
30:30They're both for health and services.
30:35Um so does this have any implications for the hospital system?
30:41Or there's not a comparable plan for the hospital system, I guess.
30:46But there we'll kind of we'll kind of we'll get to that maybe in like two slides.
30:56And yeah, I we fully realize it's like a new new spot.
31:00It's new to the policy, too.
31:02I know you told me it was coming.
31:03I'm really glad to see it.
31:08Yes, but happy to answer any other questions.
31:13But um, yeah, well, we can go to the next slide.
31:17Um, so here um, you know, this looks familiar.
31:20We have the two main components of health fund uh with health plan services on the left, county care, and um CCH on the right.
31:31So uh first starting with health plan services.
31:35Uh for so for 2026, we're estimating to be a projected deficit, uh, just under 50 million dollars.
31:44Uh this is down, uh this is down a bunch uh from the January forecast when we were initially estimating a deficit of about 117 million.
31:54So compared to the previous forecast, uh the biggest driver here the early deficit really relates on the expense side with those managed care claims coming in higher than anticipated uh to start the year.
32:10And so this has come down from the last forecast because uh like the biggest factor is making that uh continuing to continuing appropriation.
32:20Um so that uh you know, we'll have enough revenues to keep up with uh some of those uh unanticipated expenses.
32:29Um then looking at uh the health plan services chart though, you could see uh the big dip in 2027.
32:38Um, as we're anticipating uh you know, the ACA adult population being impacted uh by the OBA uh provisions far as like more frequent redetermination, more rigid work requirements.
32:53Uh you know, also in that 2027 drop off is uh the uh MLTSS population who's due dual eligible for Medicaid and Medicare coming off.
33:05Um and uh you know, the county care it it's it's begins to stabilize after and in uh 2020, but um you know you can really see the impacts uh here from OBA.
33:18Um on the health care services side on the right, this is where we're really seeing the deficits and the out years, uh similar to the last couple of presentations that we've given.
33:31Um that really has not really changed.
33:34Um but yeah, you could see we're anticipating um folks covered currently under Medicaid shifting to uh uncompensated care um that's at CCH, and that's um what's driving down uh revenues and not keeping up with uh growing expenditures.
33:59Um so now back to the CCH side that you were just kind of wondering about.
34:04So uh also 2026 budget, uh so the county established a uh an adjusted fund balance for the health for the health fund.
34:14Uh this is to help mitigate financial pressures in the out years, um, you know, any potential exposure to other uh federal policy changes that we might not be factoring in.
34:26But uh so just some background over the last couple of years.
34:30Um CCH has ended um many of the fiscal years with surplus.
34:36Um but because the health fund is an enterprise fund, CCH can't do uh like assigned reserves similar to like what we do in the uh general fund side.
34:48So beginning in 2020 fiscal year 2026, we established this adjusted fund balance.
35:00Um and so this is determined uh you know, first calculating the fund balance uh revenues minus expenditures, um, but then the adjustment part comes with deducting um pension, other post-employment benefits, um non-operating revenues such such as um uh interest income.
35:17And so that's how the we come to an adjusted fund balance.
35:21So for in the 2026 um budget, we calculate an adjusted fund balance for the health fund of about 165 million dollars.
35:31Um, you know, similar to the fund balance calculations in the general fund, this fund balance is then like overlaid with the floor and a ceiling.
35:41Um so the floor in this case is one month of expenses and the ceiling is two months of expenses.
35:48Uh and so if the fund balance, this 165 uh were to exceed the floor threshold, uh CCH would then be able, they would be able to use those funds in the following year appropriation, uh annual appropriation so 2027.
36:06Um they don't have to.
36:08Um if the fund balance were to exceed the the two months ceiling, um then that that amount above the ceiling must be appropriated in annual appropriation for the following year.
36:21Um that's one part of it.
36:23And the second part is that the county must offset that amount in the annual property tax allocation to the health fund.
36:34So um based on our uh calculations for the uh 2026 budget, you know, we have the adjusted fund balance of about 165 million.
36:45Uh the full the floor, the one month is uh uh overlaid with is about a just under 150 million.
36:53So that means that uh the adjusted fund balance um is about 16 million dollars.
37:00Uh that CCH would be able to use in fiscal year 2027 if they wanted to.
37:08Uh we currently in our forecast, we don't have that 15 million baked into the 2027 uh forecast for revenues.
37:18We don't have that in there, uh, but it would be available if uh PH were to want to include it.
37:26Um, of course, in the out years though, availability level of the funds, it would depend on how the health fund performs financially.
37:36So this is something that would be here, yeah.
37:42So for the general fund you the minimum balance requires an adjustment if you go below the minimum balance.
37:55It's not clear to me, is that the same here if they go and they're only 15 million above the minimum right now, they were well below the minimum, would it require some change operating procedures?
38:09I mean, not necessarily.
38:12I mean, hard particularly because this is an adjusted fund balance that we created for this purpose, and so it's it's it's not what's reflected in their um fund balance that's in their annual financial report exactly.
38:30So we don't yeah, we don't necessarily require that, but if they if they're if it's consistently under the floor, there would be nothing available necessarily in future years.
38:44So it kind of theoretically corrects itself, or it's it's not it's something where the idea is that this is intended to be a way to utilize some of those positive results that Ray was talking about in future years.
39:06That's kind of the goal.
39:08But um they have to produce a balanced budget regardless.
39:13So um so let me let me just try to something.
39:22So historically, there historically there has been no mechanism for us to take advantage of any positive results at the at year end.
39:33Um prior to positive results, there's just nothing to use.
39:38And so since in the last few years, we've been able to end the year positively in the health fund, but with no mechanism to take advantage of that.
39:48So this takes advantage of those positive years.
39:51But if we ever get to a place where we fall below, then we're kind of back where we were years ago with nothing to use.
40:00So this is just giving us the opportunity to take advantage of good years.
40:03So what happened to the positive fund balances in the last few years?
40:07And those were those used in the in the next years or what's what you're seeing.
40:19So it's just sitting there, it's sitting there.
40:21And and is is that I'm not I guess I'm a little confused because I thought it's an uh an entry with an enterprise fund.
40:30It couldn't do that.
40:32It couldn't have the money just sitting there.
40:34That's exactly what I was saying when we were trying to establish this.
40:38Um it's like with an enterprise fund, typically it falls to um our uh unfunded liabilities, especially where it relates to pension, right?
40:49So it's like, how are we able to do this?
40:51But when we talk to our auditors, and it's like the way you have to do that is use this HDF adjusted fund balance, number one, and number two, it's it's cash, right?
41:01So there's this cash that's been sitting there that we can use.
41:06So that's how we've been able to uh use this or establish this one.
41:11Because if you if you look at the financial statements of the of the hospital system now, the pension liabilities that they charge, the costs for the issuing of debt, all expenses that the county covers through cash transactions ourselves are captured within their financials.
41:29And so their overall liability, all their pension costs are captured at the bottom line of their expenses because they're on an accrual basis of accounting.
41:38And so it looks like they have a negative six billion dollar unassigned ending fund balance year.
41:45But over the last 10 years, what we've seen is that if you kind of strip away all of these these expenses that are actually incurred by the county itself, um, or by the by the as the downtown is as they'll they they refer to us uh and the hospital system we we pay all of those expenses.
42:07If you strip away all of that and you look over the last 10 years, what you'll find is that they actually have a fund balance that they've been they've been incurring.
42:15And so instead of allowing for that fund balance to be used against that um that unfunded or all those liabilities captured, we've kind of worked with the auditors devise this methodology, it's kind of indicated so that we can take advantage of those uh favorable values uh and appropriate them in future years instead of just paying down this this liability, which you know, in my view, um kind of um misrepresents the actual financial condition of the hospital system because it attributes liabilities to it uh that it doesn't actually pay.
42:56Okay, so this is I think a really great step forward in terms of uh making the accounting a bit more transparent.
43:10So thank you very much for doing this.
43:13It would be great if we continue to see these positive years and can continue to contribute to this.
43:18Probably not, but you saw the other slides.
43:21No, uh yeah, uh nonetheless, yeah.
43:25Uh for the long run, I think this is good, but right, you still have the problems that you have previously, or you're gonna quit very quickly have them.
43:32Yeah, is what it's well I mean, what I would say is that doesn't stop us from performing the calculation, right?
43:40That needs to be dead, and so maybe the mil that's 15 six million dollars in 2026, but maybe it's negative 70 million in the following year.
43:50But you know, maybe it'll come back again and right, and then be able to leverage those resources purposes, and we'll also have the transparency of being able to show that we had to leverage county resources in order to support the hospital because they were unable to meet the make make ends meet in this particular situation.
44:12So just to understand, so the liability short hospitals, but down time is taking care of it.
44:22So, like all of the pension costs that that are attributed to the to the to the um personnel at the hospital, for instance, are all paid out of the general funds um expenses.
44:39So that liability, the total liability of the pension personnel is a bottom line statement on their balance sheet um that they have to attribute to their expenses, but they don't actually make that payment, just as an example.
44:55There's another there's other couple other ones, all the debt service um that they incur is also paid for uh by the general fund.
45:00All the debt service that they incur is also paid for by the general fund.
45:04So any interest or principal that could be attributed to them are captured within their financial statements, but the county is the one that actually pays the bill for those particular expenses via the debt service expense account within the council.
45:18Yeah, so that's problem down the road in terms of making the financial statements clear.
45:24And so I mean, at least we have this metric now that we can leverage for the purpose of kind of leveraging those those positive years for um appropriations.
45:46Thanks, uh team, for adding more colors to that.
45:51So yeah, here next slide here.
45:53We have uh a look at county care membership.
45:56Um we made a change uh from our project slides of how we showed this.
46:04Um we essentially broke out here in the blue bars the uh the ACA adult population.
46:12Uh really just to highlight um it's so it's easy to see the uh the impact of the anticipated impact uh of Oba kicking in and how this would um uh just have a decline, anticipated decline in the ACA adult enrollment here starting in January of 2027.
46:36Um and so you know, the the gray bars, uh, the other the other populations is you know, relatively relatively flat, minimal declines, but um, you know, uh the county care membership projections, you could see um the decl the overall declines mostly driven from the uh anticipated over impacts on the ACA groups.
46:57Um, you know, as we mentioned in previous um iterations of this, the um MLTSS population, that dual eligible group, uh they're anticipated to uh no longer be covered as of January 2027.
47:14Uh so they're gonna be removed from the county care.
47:17Um, and then one other update is that um our membership projections here have health benefits for immigrant seniors um turning off in July of 2028, uh, which aligns with the state's fiscal year, uh fiscal year 2029.
47:36So what is have you seen anything or is the hospital seen anything in terms of uninsured people showing up since the emigrant also kicked off?
47:47Uh well, there has in the last couple of I guess like the last quarter to the last six months, there has been a shift um of more self-pay on CCH side from those covered in Medicare.
48:04It hasn't been drastic, but we we have started to see it as far as like what the payer mix looks like.
48:11Um I think we'll probably need a couple more months of data just to see if it's not like I guess like a blip or one-off, but um we are starting to see more shifts to uh self-pay as far as folks um don't not getting covered.
48:31Um, I don't know if anybody else knows.
48:33Um, are we also starting to see more usage of folks that are on county care?
48:39It seems to be trying to get all the care they can before they lose it.
48:43So we're also seeing an uptick.
48:46Yeah, there was an up, there was a big uptick that CCH team towards the end, the latter half of 25.
48:57Um, and now it's too what's was really driving those those claims that were then hitting us in December and January, uh, which probably I'd tap into like those those that cash reserve.
49:10But it seemed like in more recent uh periods that um as far as claims expenses go that has leveled out to more um uh I guess like what we've seen in past years, what we might expect closer to like uh uh the budget spread.
49:29Um, but I think maybe like with news breaking at the end of the at the end of 2025, that kind of sent people uh to go seek out services.
49:41So uh might be asking for something that's not doable, but um I'm wondering if we could have a sort of parallel or analogous chart for health care services in terms of a distribution of the population among different types.
50:00So there's a medic, a Medicaid population, there's a self-pay population within the Medicaid, we might be able to break that out and also projections.
50:15Be able to get that.
50:16But that I think that's a big concern is what are what are the projections of those populations?
50:22You're referring to like people that are coming into the hospital or that are on the plan.
50:27Well, I don't know what's possible to do, but uh ideally it would be the the health plan, the health care services relation beyond not only the hospital but the clinics as well.
50:39Yeah, ideally like a breakout of like the NPSR, the patient service revenue by these groups, something like that.
50:48And then in particular, to what extent can you project them?
50:53And so it's that's easier to do for the county care membership, yeah than it is for the and are you thinking this would be kind of the based off of the dollar amount we're getting, or based because we certainly have that or based more off of kind of some other metric of utilization.
51:15Uh, because I mean if you can do it with dollars, that's that's it's good.
51:20Um I I just finished a or we have it still in draft, a paper where we're trying to do this kind of for the state.
51:26What are the financial implications of Oba?
51:30And you know, what we did, I didn't do it, somebody else in the paper did it, but he just did a projections by the different types of populations of what what's gonna happen.
51:40So who's gonna fall off of Medicaid basically and what's that gonna do to state revenues?
51:48I will say I'm not sure if this is what you're asking.
51:50We don't have a specific way of breaking out the hospital's Medicaid revenue based off of kind of like the different Medicaid populations.
52:03Oh, you don't know, but however, the way well, Ray could probably add more that we made assumptions about you know how it would drop off in the uh forecast, but no, we don't have it quite like that.
52:16Yeah, I don't know if you have yeah, we we might be able to put something together based up off based off of how we do our scenarios for netpatient service revenue or like the payer groups.
52:29Um but yeah, to what Lindsay's point was as far as like seeing it comes, we don't have like a breakouts like on like an account level on the revenue side to be able to see like the actuals to to easily determine that.
52:48Well, can back some of trying to say earlier.
52:53Can I know that you couldn't do it for confidential confidentiality reasons, but can they figure out what happened to the immigrants?
53:04Or were they showing up if they're showing up somewhere else in the system?
53:09Um if so, where we'd have to double, we'd have to check on that to see if um they have I mean I'm sure they wouldn't use yeah, yeah, but if that's something that they uh that might help forecast what might happen with some of these other groups I mean, one of the the issues we faced in the work I was doing was it looks like the people that are gonna get knocked off are mostly the expansion population.
53:42The expansion population is uh first of all, more of them are probably gonna get employer sponsored health insurance.
53:48They're also relatively healthy, they aren't the most expensive populations.
53:53So looking just at the drop in population is uh, I mean that there were all kinds of things, but in terms of the state, those people are matched at 90 at 90 percent.
54:08So the state's not getting much back by knocking them off of Medicaid, but they're also I don't know.
54:15They're less costly, they may be less costly to service if they become uninsured.
54:21I'm not sure if that's true.
54:22Well, I mean, is is there any data that would that you could compare and see if the profile of the lighter blue people are is close to the orange people?
54:34And then you can then try to find out what's happened to the orange people.
54:39Because the the yellow people are clearly different.
54:45And the dark blue population are clearly different.
54:50But maybe there's some correlation between the light blue and the orange, and if you had that on the orange, you could refine the forecast for the blue.
55:05I I guess big picture.
55:08What I'm asking for is to what extent can we do projections like this for the health uh health care services kind of thing.
55:24They can tell you kind of how their uncompensated care has increased over the last few months, right?
55:31And tell you a little bit about what the typepayer types are.
55:37I don't think we have that information embedded in the chart of accounts or the way that we capture the revenues, but I think it's information that they have.
55:46Yeah, we I mean, yeah, we yeah, we have um we have we have enough information to kind of know growth and uncompensated and shifts with Medicaid, but yeah, we don't necessarily not be able to make a chart quite like this that is based on actual reality, it would have to be based off of assumptions.
56:10Yeah, and it's based on and it'll also be based off the claims that are processed at the time, which might not necessarily match up to the actual membership, right?
56:18So like another piece to think about, right?
56:20Is that there's a timing?
56:22There's a timing difference, right?
56:23That's part of the reason why we need to have the reserves in place too, right?
56:27Because we can see the declines in in um revenues don't match up with the declines in claims, right?
56:36So right now, as membership declines go down or upside down with claims going up and and membership uh reimbursements going down.
56:48So I mean, you know, there is a certain level of predictability that you can expect, I would think from the um declines in membership having an impact on your uncompensated claims, right?
57:03But that's gotta work its way through the system.
57:05There's like a lag three, six months, right?
57:08I mean, you paid pro you paid a hospital bill before, right?
57:13You know, six months, six months isn't you get it.
57:18Yeah, so it's gotta work through all of that, right?
57:29Appreciate the suggestion though.
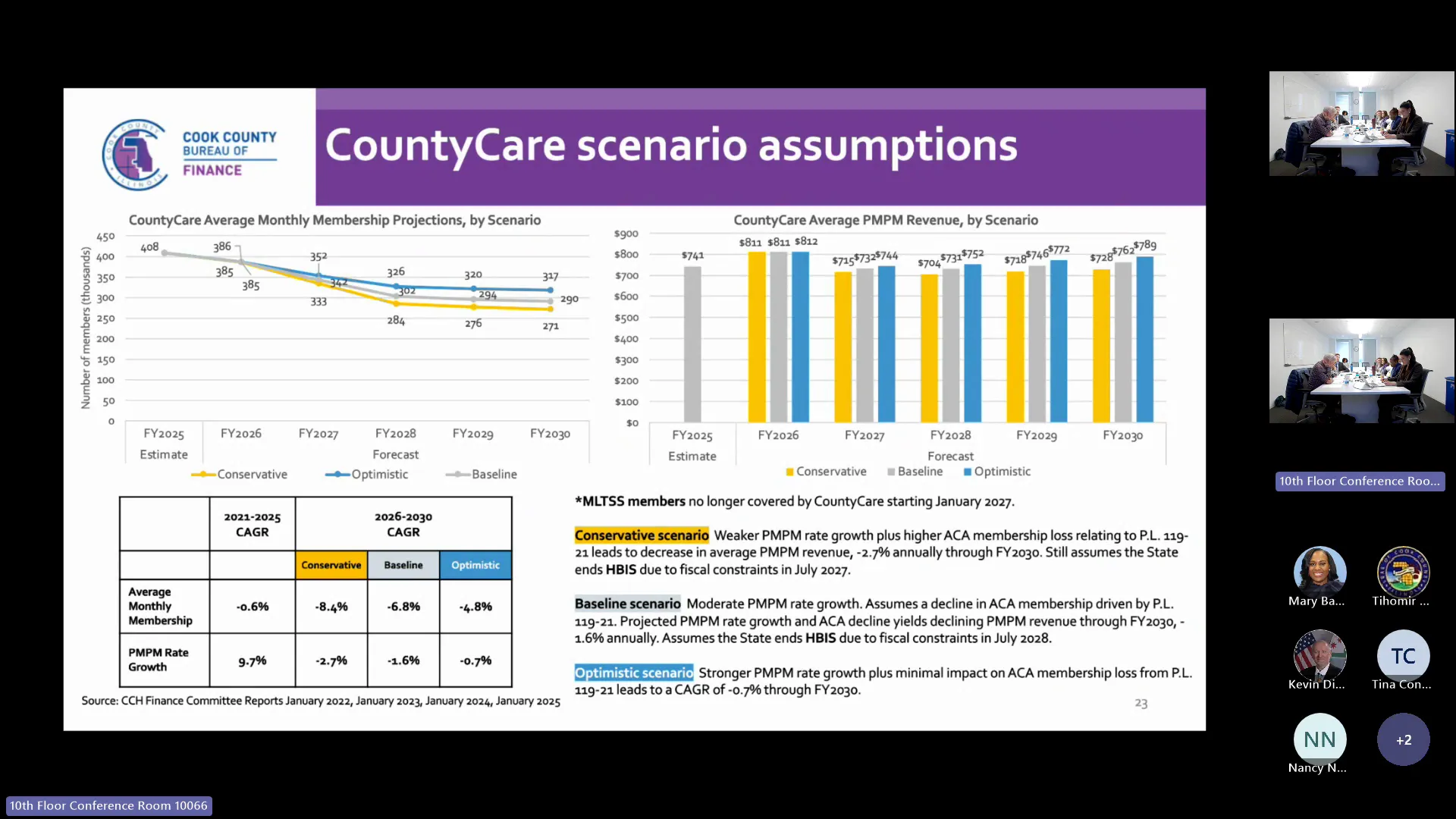
57:33Uh just so just wrapping up, uh slides here on county care, but um of our different scenario assumptions here.
57:42So um on the chart on the left, uh, we have uh our difference our three different scenarios playing out for uh membership projections.
57:52Um so you know, really in all all three revenue, uh excuse me, we're really in all three membership projections here.
58:00Uh, we're anticipating uh declines uh in membership um into uh this year 2030.
58:09Um, in the baseline and conservative scenarios, we're we're assuming that the state will end uh those health benefits for immigrant seniors.
58:19Um difference is like in the optimistic scenario, the um county care is anticipating that the uh health benefits for immigrant seniors will remain in there.
58:30Um but uh really the the drop-offs are um are just they just have different scenarios playing out of how the intensity of uh OBA those OVA provisions impacting the ACA adult population.
58:47Um and then on the chart on the right, uh this is the so the average um per member per month revenue uh across the the populations.
58:57So we're seeing a uh a significant decline uh from 26 into 2027.
59:05Uh and so you know, just something to consider here is that the average uh per member per month uh revenue, it's it's very sensitive to um varying per member per month rates in the in the enrollment mix.
59:20Uh so for example, a large reduction um in membership population that has a higher reimbursement rate will have uh a significant impact on this average PMP revenue.
59:35So, you know, as we've stated before, we have the uh MLTSS population coming off uh the enrollments starting in 20 starting in calendar year 2027.
59:46Uh so they they have a high reimbursement rate.
59:49So with them coming off, that's what's really driving the the noticeable drop here in 2027 compared to 2026.
1:00:00Um, but then you know, with um different uh growth rates applied to the uh to the PMPM rates across the baseline optimistic and conservative scenarios, we're seeing um some some growth uh going into the out years from an average PMP uh revenue view.
1:00:21Um and then so on the on the next slide, uh building on the assumptions.
1:00:26Um here's what we have for county care revenue overall.
1:00:31Uh, perhaps unsurprisingly, we're seeing a sizable decline in 2027 uh with the impact of OBA on membership overall.
1:00:41Um that's across all three scenarios.
1:00:44Um again, it's just um, you know, the difference in the scenarios here is really um driven by the different impacts um assumed across the three scenarios from OBA.
1:00:57So in the optimistic uh case, for example, you know, anticipating less of an impact on that ACA adult population.
1:01:05Um however, if you if you do look at the optimistic case though, um, you know, even all the way out to 2030 uh revenues, they don't they don't reach uh the 2026 levels at the current assumptions.
1:01:22Um so we're anticipating a pretty large um impact county care side here from those uh provisions.
1:01:34Um so hopping over now to the CCH um specifically with patient service revenues.
1:01:42Um so right now uh similar to previous um uh updates to this forecast, we're assuming uh some shifts as far as the pair mix goes from those individuals covered by Medicaid uh going to self-pay and uninsured.
1:02:03Um and we're assuming that in all three scenarios here.
1:02:07Um, you know, if more patients become uninsured, that could impact um our volumes, uh the gross charges for the forecast, but we we still haven't made any adjustments to that.
1:02:19We're gonna wait and see how that uh maybe maybe pans out down the road before making adjustments or for uh feedback from the CCH team on that.
1:02:30Um but I'll just uh look at the the baseline scenario here.
1:02:35But that so we're assuming you know, consistent patient volumes growth.
1:02:39That's like the outlined of the gray bar uh growing about 1% a year into the out years.
1:02:47Um then assuming a stable coverage patterns um reimbursement rates or the collection rates remaining flat into the out years.
1:02:57Um and then on the the chart here on the on the right, this is the the projected collection rates.
1:03:04We've referred to them as yields in the past.
1:03:07So for 2026, net patient service revenue as anticipated to have a um total yield or collection rate of about 24%.
1:03:17We're anticipating that for the baseline scenario to decline to about uh 20.6% in uh fiscal year 2030.
1:03:27This is mainly again because of uh individuals covered by Medicaid that would get reimbursed shifting over to uh the much more uh less collection rates, smaller collection rates of um those uh self-paid population.
1:03:53And then uh so on the next slide.
1:03:56Um here we have a um uh kind of like an overview of collection rates.
1:04:03Um so we we brought this, we added this slide in the last presentation just to kind of give some background of what collection rates have looked like overall for net patient service revenue.
1:04:17Um, we tried to break it out two by like the three main payer groups with Medicaid, Medicare and the private payers.
1:04:26Uh, and we also have the collection rates uh overall with uh the impact of adding in directed payments, uh, which uh helps supplement safety net hospitals that have large uh Medicaid um populations.
1:04:43Um so you know, we overall have seen declining collection rates across most of the payer groups and for the collection rate overall.
1:04:53Um, you know, there's some there's some different factors play in play here.
1:05:00It's hard to nail down exactly uh what's driving it, because um, you know, there are some things which uh you know Dean kind of touched on earlier as far as like there being a lag and when we would get reimbursed for some of these payers.
1:05:13Um, you know, uh the CCH team for 2026 anticipates the uh yields or collection rates to increase uh for some of these groups, uh primarily for Medicaid and Medicare, um, which are uh typically have more make up more of the gross charges for net patient service revenue.
1:05:36Um so yeah, the CCH team anticipates that in 2026 we'll see an uptick in those collusion rates for the Medicaid groups and Medicare groups, uh, but the private payers group, which does include like the commercial um commercially insured folks, uh, but also include that self-pay population.
1:05:58So as there's more of a shift um from folks who are on Medicaid going into self-pay, you know, the the self-pay uh broken out on the uh table on the right there, you could see the you know, you know, around one percent of that is collected from gross charges.
1:06:16So that's what's really bringing it down in um uh year over year.
1:06:21Why do they think it's gonna go up for Medicaid Medicare?
1:06:25Uh well, I think one part of it too is just um uh there may have been a lag in 2025 as far as re changes to reimbursements and that maybe coming through in 2026.
1:06:38Um another part of it as well, it's like the denominator with like the gross charges um is is impacting it too as far as like how it's how that percentage is calculated.
1:06:53Um but just you know, uh overall they just they're anticipating it to increase by 26.
1:07:03So we can we could try to get some more details from them, uh, especially as we get maybe a couple more months of uh data for the fiscal year to see if that trend's keeping up uh or if it's trending towards that, you know, for Medicaid in this case 27% and Medicare 40%.
1:07:24Am I remembering that there was some big collection activity that were resources were allocated to try to increase collections around 2023?
1:07:36Yeah, there's been a number of uh initiatives done at CCH to try to increase collections and improve the revenue cycle.
1:07:47And yeah, I do think, yeah, that is I think to some extent driving some of what you may be seeing, yeah, like 23, 24.
1:07:57Um some of those items theoretically would kind of continue into current to have existing operations, but then some items may have resulted in some one time.
1:08:09Well, that's and I'm wondering if there's any role to clean that out to see because I seem to remember there was some big initiative that happened when I first started hanging out with you guys.
1:08:22And if you could strip off the one the stuff that was clearly from several way beyond the normal collection rate, just to see is 40 really normal, 40 percent in for Medicare.
1:08:38And then it just looks like it's relatively little without period because there's a bunch of kinds.
1:08:49My understanding is that one of the ways one of the things you can do is you can get self-pay people signed up for Medicaid in some cases, I suppose, Medicare.
1:09:01And we don't really see any of that, what's going on with that in the chart.
1:09:06I don't know if there's any way to capture that, but but I mean right, the self-pay basically probably they can't pay it, they just don't have the money to pay it.
1:09:17So there's no point in going after them to try and get them to pay.
1:09:22But what we might be able to do is get the paperwork filed so that we get them one of the government insurance programs.
1:09:30That's usually done when they present themselves at the hospital when they go to say, okay, you don't have insurance.
1:09:37Okay, we we have insurance for you.
1:09:41And so like qualifying for in a way, like that's probably got more potent potential.
1:09:48And I don't know how well they're doing, or I don't know if if they're if more can be done there, but like I'm not I'm not optimistic.
1:09:56Self-pay is you know, trying to get people to self-pay is going to do it good, right?
1:10:02Unless you convert them to being covered by something.
1:10:06Yeah, whoever we converted is kind of already captured in Medicaid.
1:10:11I think we assume Ray, what we assume in the forecast, 50% of them get of the folks who show up to who may who we try to sign up, wind up getting converted.
1:10:26Okay, so I mean I think one thing that would be interesting to me, I don't I don't know what we can do with it, would be to have some data about like what's going on, how's that go?
1:10:35How is that happening over time?
1:10:37Yeah, and then you know because certainly there are I mean, I'm sure there are people that know administrative procedures that can make these effective, right?
1:10:52This is not rocket science, right?
1:10:56People have been working on this for years.
1:10:59Yeah, and it wouldn't it would not increase collection rates.
1:11:04That's fine, but it would it would kind of change the uh the shift would shift folks from uncompensated to Medicaid.
1:11:14Yeah, which is which is uh means that they would play into those rates there.
1:11:21My understanding also is that under the one big beautiful bill, there's like a retro, they modified the retroactive, like uh like how quickly, like if you sign up for Medicaid, instead of it being 90 days look back, it's a 30-day look back.
1:11:38Right, right, right.
1:11:39So that's painful too, right?
1:11:41It's painful as well.
1:11:42So yeah, but again, it means I guess it means if somebody comes in with a problem, you want to move as quickly as you can so that you get the paperwork through.
1:11:53So that could be a change in procedure that could help.
1:12:05Um, and then uh so one last slide here on on the health plan.
1:12:10Um, you know, looking at health care services, uh different scenarios here.
1:12:15Um really what we highlight on this slide is the uh yellow bars on top, which is um dish, the disproportionate share hospital revenue.
1:12:27Um so right now the baseline and the optimistic scenarios are assuming that there's not gonna be any um out year cuts to dish funding, uh, which was you know a topic of discussion at the last couple of meetings as far would we see that happen in 26, 27, and 28.
1:12:51Um so right now, uh, you know, based off of uh recent uh legislation on the federal level, um the dish cuts have been delayed until um uh the start of I believe fiscal year 2028.
1:13:06So we have here reflected in the conservative scenario.
1:13:10Um if Dish were to see cuts, um, we would see the impacts um up top top on the yellow bars for the conservative scenario.
1:13:20Um and that would begin in our fiscal year 2027 just because of the overlap of the the federal fiscal year and the county's fiscal year.
1:13:29Um, but currently uh, you know, we've updated also our just in general our dish forecast for 2026.
1:13:37Uh it was adopted at about 200 million dollars, so we've updated it to about 236 million uh based off of the uh the the monthly fixed payments that we that we get from the state so uh apologies for any other last questions for the health general health fund forecast updates.
1:14:14All right, thank you.
1:14:15The next item on the agenda is public comment.
1:14:17Loma, do we have any public speakers?
1:14:20Yeah, we have no registered public speakers.
1:14:23All right, do we have any public speakers registered in the virtual chat box?
1:14:27Here that we have no registered public speakers in the chat box.
1:14:30All right, then the next item on the agenda is a German.
1:14:33Is there a motion to adjourn?
1:14:36So is there a second second?
1:14:40All right, the motion to adjourn has been moved by Commissioner Merriman and seconded by Commissioner Davila.
1:14:46All of those in favor signify signify by saying aye.
1:14:49All of those opposed signify by saying nay in the append of the chair, the ayes have it.
1:14:54The next meeting is adjourned.
1:14:55The next meeting is scheduled for Thursday, June 25th, 2026, 2026 um at 5 30 p.m.